
Adult and Pediatric Urologist, Urooncologist, Endoscopic, Laparoscopic and Robotic Surgeon, Andrologist and Transplant Surgeon
MBBS, MS, DNB, FCPS, MRCS (UK), MNAMS, MCH (Urology, India), FICS (USA), FACS (USA), FECSM (European Board), DLS (EITS, France), FRCS (Urology, UK, JSCFE Gold Medal), Fellowship In Endourology, Urooncology, Robotic Surgery (Australia)
This section highlights the normal functions of the important urological organs.
Most individuals have two kidneys, each about the size of a fist, located on either side of the spine at the lowest level of the rib cage. Sometimes, it may be absent from birth. Each kidney contains up to a million functioning units (filtering units) called nephrons.
The kidneys perform their life-sustaining job of filtering and returning to the bloodstream about 200 quarts of fluid every 24 hours. About two quarts are removed from the body in the form of urine, and about 198 quarts are recovered. The urine we excrete has been stored in the bladder for anywhere from 1 to 8 hours.
What is the role of kidneys?
The kidneys perform the following functions:
What are common causes of Chronic Kidney Disease (CKD, also called Renal Failure)?
CKD is a condition where kidneys don’t work properly for 3 months or longer. Diseases such as Diabetes, Hypertension, High Cholesterol, Glomerulonephritis, Kidney infections, neglected large kidney stones, Inherited Diseases, long term usage of certain pain killers (NSAIDs) are common causes of CKD. It is diagnosed by doing blood and urine tests.
What is the bladder?
The bladder is a storage organ that sits in your pelvis. Urine is made by your kidneys and stored in the bladder until you are ready to empty it. When you go to the toilet your bladder outlet muscles (urethral sphincter and pelvic floor) relax and your bladder contracts (squeezes) emptying your bladder of urine. Your brain controls your bladder by sending messages to tell it when to hold on and when to empty.
What are the signs of a healthy bladder?
A normal bladder:
If you are worried about your bladder or have been instructed to consult a urologist by your GP, you can book an appointment. Please visit the resources to learn more about your particular Bladder Problems and Available Options
What are common causes of Chronic Kidney Disease (CKD, also called Renal Failure)?
CKD is a condition where kidneys don’t work properly for 3 months or longer. Diseases such as Diabetes, Hypertension, High Cholesterol, Glomerulonephritis, Kidney infections, neglected large kidney stones, Inherited Diseases, long term usage of certain pain killers (NSAIDs) are common causes of CKD. It is diagnosed by doing blood and urine tests.
The prostate gland is located just below the bladder in men and surrounds the top portion of the tube that drains urine from the bladder (urethra). The prostate's primary function is to produce the fluid that nourishes and transports sperm (seminal fluid).
What are common problems with prostate?
Benign prostate hyperplasia (BPH, non-cancerous enlargement of prostate), Prostatitis (inflammation/ swelling of the prostate) and Prostate cancer (second most common cancer in men) are common conditions that affect the prostate.
Testicle or testis (plural testes) is the male reproductive gland. Each testis is attached to the body wall by a thin cord called the spermatic cord, which is connected to the abdomen. The testes produce testosterone, the primary male sex hormone, and sperms.
What are common problems with testis?
Common problems affecting testis are epididymitis (inflammation of epididymis, a tube which rests alongside testis and stores sperms), orchitis (inflammation of testis), hydrocele (fluid collection around testis), torsion (an emergency condition where the testicular blood supply is lost due to twisting of spermatic cord, a structure that suspends the testis in the scrotum), varicocele (enlargement of veins in the scrotum that may affect sperm quality and fertility), testis cancer.
What is BPH?
Benign prostatic hyperplasia (also called BPH) is a condition in men in which the prostate gland is enlarged and not cancerous. The prostate is a walnut-shaped gland that is part of the male reproductive system. The prostate's primary function is to produce the fluid that nourishes and transports sperm (seminal fluid). Prostate fluid is essential for a man’s fertility.
As the prostate enlarges, the gland presses against and pinches the urethra. The bladder wall becomes thicker. Eventually, the bladder may weaken and lose the ability to empty completely, leaving some urine in the bladder.
What causes BPH?
Throughout their lives, men produce testosterone, a male hormone, and small amounts of estrogen, a female hormone. As men age, the amount of active testosterone in their blood decreases, which leaves a higher proportion of estrogen. Higher proportion of estrogen within the prostate increases the activity of substances that promote prostate cell growth.
Another theory focuses on dihydrotestosterone (DHT), a male hormone that plays a role in prostate development and growth. Older men continue to produce and accumulate high levels of DHT in the prostate. This accumulation of DHT may encourage prostate cells to continue to grow.
How common is BPH?
Benign prostatic hyperplasia is the most common prostate problem for men older than age 50. Benign prostatic hyperplasia affects about 50 percent of men between the ages of 51 and 60 and up to 90 percent of men older than 80.
Who is more likely to develop BPH?
Men with the following factors are more likely to develop benign prostatic hyperplasia:
What are the symptoms of BPH?
Lower urinary tract symptoms suggestive of benign prostatic hyperplasia may include
The size of the prostate does not always determine the severity of the blockage or symptoms. Some men with greatly enlarged prostates have little blockage and few symptoms, while other men who have minimally enlarged prostates have greater blockage and more symptoms. Sometimes men may not know they have a blockage until they cannot urinate. This condition, called acute urinary retention, can result from taking over-the-counter cold or allergy medications that contain decongestants, such as pseudoephedrine and oxymetazoline.
What are the complications of BPH?
The complications of benign prostatic hyperplasia may include
Most men with benign prostatic hyperplasia do not develop these complications. However, kidney damage in particular can be a serious health threat when it occurs.
When to Seek Medical Care?
A person may have urinary symptoms unrelated to benign prostatic hyperplasia that are caused by bladder problems, UTIs, or prostatitis—inflammation of the prostate. Symptoms of benign prostatic hyperplasia also can signal more serious conditions, including prostate cancer.
Men with symptoms of benign prostatic hyperplasia should see a health care provider. Men with the following symptoms should seek immediate medical care:
How is benign prostatic hyperplasia diagnosed?
A health care provider diagnoses benign prostatic hyperplasia based on
How is benign prostatic hyperplasia treated?
Treatment options for benign prostatic hyperplasia may include
Your healthcare provider (urologist) chooses the type of treatment based on the severity of symptoms, how much the symptoms affect a man’s daily life, and a man’s preferences.
What are Kidney Stones?
Kidney stones are hard deposits made of minerals and salts that form inside your kidneys.
What causes Kidney Stones?
Kidney stones form when your urine contains more crystal-forming substances — such as calcium, oxalate and uric acid — than the fluid in your urine can dilute. At the same time, your urine may lack substances that prevent crystals from sticking together, creating an ideal environment for kidney stones to form.
What factors can increase the risk of kidney stone formation?
Factors that may increase your risk of developing kidney stones include:
What are the types of kidney stones?
Types of kidney stones include:
Knowing the type of kidney stone you have helps determine its cause, and may give clues on how to reduce your risk of getting more kidney stones. If possible, try to save your kidney stone if you pass one so that you can bring it to your doctor for analysis.
What are the common symptoms of kidney stones?
Small kidney stones can usually pass on their own without causing any discomfort. Larger stones can get stuck in the ureters (the tubes through which urine flows from kidneys to bladder), which leads to intense discomfort. When a stone gets stuck in a ureter, it blocks the flow of urine and causes severe pain.
The following symptoms may be experienced when a kidney stone moves out of kidney:
If someone is experiencing these symptoms they should visit the medical practitioner immediately for further evaluation.
What are the common tests for detecting kidney stones?
If your doctor suspects that you have a kidney stone, you may have diagnostic tests and procedures, such as:
Imaging tests may show kidney stones in your urinary tract. Ultrasound, a noninvasive test that is quick and easy to perform, is often the first advised test to diagnose kidney stones. Simple abdominal X-rays are used less frequently because this kind of imaging test can miss small kidney stones. Additionally, about 20% of kidney stones are not seen in X-rays, which are called radiolucent stones.
High-speed or dual energy computerized tomography (CT) may reveal even tiny stones. This test is considered the best test to diagnose kidney stones.
MRI is not the test-of-choice in detecting kidney stones (it misses nearly 80% of kidney stones). However, in certain conditions like pregnancy, CT scan is contraindicated and MRI is the only available imaging modality that may be offered apart from ultrasound.
What are the treatment options for kidney stones?
Medical management is available to aid in the passing of small stones and for ongoing management of stones. Medications like alpha-blockers can help passing stones that are stuck in the lower part of ureter (close to the urinary bladder).

Oral alkalinization can be used to increase urine pH and dissolve uric acid stones. Periodic surveillance with imaging modalities is necessary to ensure treatment success or to guide further changes to the treatment plan.
For large stones, obstructing stones and stones that do not pass despite medical management, the following surgical options are available:
What are the suggested preventive measures for kidney stones?
One of the best preventative measures against kidney stones is proper fluid intake. It is recommended that you drink at least 8 glasses or 3 liters of water each day in order to pass about 2.6 quarts (2.5 liters) of urine daily. Other general diet and prevention recommendations include:
Based on stone analysis and metabolic work-up studies of an individual, your doctor can provide a dedicated stone prevention protocol for each individual.
UTI is an infection in any part of your urinary system — your kidneys, ureters, bladder and urethra. Most infections involve the lower urinary tract — the bladder and the urethra. Women are at greater risk of developing a UTI than are men.
What are the risk factors of UTI?
Urinary tract infections are common in women, and many women experience more than one infection during their lifetimes. Risk factors specific to women for UTIs include:
Other risk factors for UTIs include:
What are the common symptoms of UTI?
UTI may be completely silent and picked up at urine test. Common complaints include:
UTIs may be overlooked or mistaken for other conditions in older adults.
What are the complications of UTI?
When treated promptly and properly, lower urinary tract infections rarely lead to complications. But left untreated, a urinary tract infection can have serious consequences.
Complications of a UTI may include:
What are suggested prevention measures?
You can take these steps to reduce your risk of urinary tract infections:
The urethra is a thin tube through which the bladder empties urine out of the body. The female urethra is much shorter and wider than in males. Male urethra is about 15-20 cms long and transports sperms along with urine through the penis outside. When a scar from swelling, injury or infection causes urethral narrowing, it is called a urethral stricture.
Clinical relevance of Male and Female Urethra
The long and curved course of male urethra makes urinary catheterization (the process of inserting a tube through the urethra and into the bladder, typically performed in situations where urine output needs to be monitored (such as sepsis), or when the patient is unable to pass urine (urinary retention)) a complex procedure. In male urethra, there are two angles to consider during catheterization, the infrapubic prepubicangles and the prepubic angle can be diminished by holding the penis upwards during urinary catheterisation.

Due to the short length of the urethra, women are more susceptible to infections of the urinary tract. This usually manifests as cystitis, an infection of the bladder.
What are the causes of Urethral Stricture?
Men are more likely to have a urethral stricture because of their longer urethra. They are rare in women and in infants.
Common causes are:
In many cases, no cause can be found.
What are the common symptoms of Urethral Stricture?
The urethra is like a garden hose. When there is a kink or narrowing along the hose, no matter how short or long, the flow is reduced. Urethral stricture most commonly leads to slow or decreased urine stream. Problems with urinating, UTIs, and swelling or infections of the prostate may occur. Severe blockage that lasts a long time can damage the kidneys.
Other symptoms are:
What are the common diagnostic tests?
The commonly utilized tests are:
What are the available treatment options?
The treatment options depend on the extent and severity of stricture. Treatments include:
There are no available drugs to help treat strictures.
Without treatment, one will continue to have problems with voiding. Urinary and/or testicular infections and stones could develop. Urine retention may occur, which could lead to an enlarged bladder and kidney problems.
What are the suggested measures for Prevention?
Kidney cancer is the ninth most commonly occurring cancer in men and the 14th most commonly occurring cancer in women. Renal cell carcinoma (RCC), also known as renal cell cancer or renal cell adenocarcinoma, is the most common type of kidney cancer (about 9 out of 10 kidney cancers). They arise from structures called Renal Tubules which filter fluids in the kidney before the waste (urine) is discharged into the bladder. About 5 to 10 percent of kidney cancers are Transitional cell cancers (TCC). These don’t start in the kidney itself, but in the lining of the renal pelvis (where the ureters meet the kidneys). These are usually more aggressive than RCCs. Most people diagnosed with kidney cancer are between 65 and 74. Kidney cancer is twice as common in men than in women, and African Americans, American Indian and Alaskan Natives are more likely to be diagnosed.
What are the risk factors for RCC?
The following risk factors have been associated with RCCs:
How is RCC diagnosed?
Many early kidney cancers are discovered during testing for other reasons. A urine sample may show blood, or a blood test may detect anemia. An imaging study of the abdomen for unrelated symptoms may reveal kidney cancer.
If doctors suspect kidney cancer, imaging studies are important for diagnosis. In some cases, kidney cancer may be diagnosed with imaging studies alone.
These include:
If surgery is recommended, the diagnosis also may be confirmed post-op by looking at cancer cells under a microscope, called pathologic diagnosis. Kidney cancer also may be confirmed with a needle biopsy.
Learn more about diagnosing kidney cancer
What are the treatment options available?
Surgery is the first-line treatment option for most patients with renal cell carcinoma. Other treatment options for all types of kidney cancer include:
Prostate cancer is the most common cancer and the second leading cause of cancer death among men in the United States. The American Cancer Society (ACS) estimates that about 248,530 new cases of prostate cancer will be diagnosed in 2021. Prostate cancer usually grows very slowly, and finding and treating it before symptoms occur may not improve men's health or help them live longer.
Some prostate cancers are aggressive. Approximately one in every 41 men diagnosed will die from the disease, according to the ACS. Black men are reportedly more prone to developing fast-growing prostate cancers that start causing problems earlier and are harder to treat.
What are the risk factors of prostate cancer?
Prostate cancer is rarely diagnosed in men younger than 40. By age 50, men undergo changes in the size and shape of the cells in the prostate. Understanding whether these changes are signs of a tumor and knowing your risk for developing prostate cancer are important steps in protecting your health.
Besides age, other risk factors for prostate cancer include:
What are the common signs and symptoms of prostate cancer?
In the early stages, prostate cancer usually doesn't show symptoms. However, as prostate cancer grows, it may lead to:
Patients who develop new or concerning symptoms should consult with their doctor or urologist.
Learn more about the signs and symptoms of prostate cancer
How is Prostate Cancer diagnosed?
Symptoms are often absent in the early stages of prostate cancer. Many cases are discovered through routine screening tests. Getting screened for prostate cancer is an individual decision. It may help to discuss the risks and benefits with a doctor.
Screening for prostate cancer usually involves the following tests:
If either of these suggests the possibility of prostate cancer, doctors typically perform additional tests before making a diagnosis.
The only way to know for sure whether a tumor is cancerous is by examining cells under a microscope, a procedure also known as a prostate biopsy.
Learn about diagnostic procedures for prostate cancer
What are the treatment options?
Deciding on prostate cancer treatment is a personal decision made between a patient and his care team. Factors such as preferences, age, health history and the cancer stage all play a role in the decision-making process.
Treatment may involve one or a combination of these options:
Other therapies that are used less commonly, or are not considered standard treatment for prostate cancer, include:
Testicular cancer most often begins in germ cells (cells that make sperm). It is uncommon and is most frequently diagnosed in men ages 20 to 34. Most testicular cancers can be cured, even if diagnosed at an advanced stage.
What are the risk factors?
These include:
Of the factors associated with the risk of developing germ cell tumours of the testis, cryptorchism and malignancy in the contralateral testis are by far the strongest. Testicular microlithiasis, vasectomy, and scrotal trauma are not risk factors for testicular cancer.
What are the common symptoms of testicular cancer?
The common symptoms of testicular tumor are:
How is testicular cancer diagnosed?
Patients should seek an urgent consultation if they suspect abnormalities in the testis. The common diagnostic tests are:

What are the treatment options?
Management is dependent on the type of tumour and stage. Approximately 90% of patients classified as having a good prognosis achieve a durable complete remission with treatment. Even metastatic disease should be seen as potentially curable. When treating young adults with a highly curable disease, possible long-term toxicity of treatment is an important consideration. Following confirmation of a germ cell tumour, all patients should be referred to a specialist centre for the management of testicular tumours.
Where possible, a radical orchidectomy should be performed. A testicular prosthesis should be offered to all patients. When appropriate, sperm storage should be offered to men who may require chemotherapy or radiotherapy.
Patients with metastases where the diagnosis is not in doubt (high tumour markers and the presence of a testicular mass) should be referred for immediate chemotherapy
Do patients need follow-up after treatment?
All patients post treatment of testis cancer will need a strict follow-up. Your doctor will schedule you for regular visits after treatment to see if the cancer has come back (recurrence). Visits may include a physical examination, blood tests, chest x-ray, and/or a CT scan to look for new tumors. Visits are usually more frequent just after treatment ends. Follow-up typically continues for at least 5 years. If there is no recurrence, you do not need further treatment.
Examining your testicles is easy
Examine your testicles regularly (Fig. below), especially if you have a risk factor for testicular cancer.
The best time to examine your testicles is right after a hot bath or shower. The scrotal skin will be relaxed, and the testicles can be felt more easily. It takes only a few minutes.
Do the exam standing:
If you find a lump, swelling, or other change, see you doctor. Changes are not always cancer, but if it is cancer and you catch it early, you have the best chance of cure.

Bladder cancer is a common type of cancer that involves the bladder. Most often the cancer starts in the cells (urothelial cells) that line the inside of your bladder. Urothelial cells are also found in the kidneys and the tubes (ureters) that connect the kidneys to the bladder. Urothelial cancer can also happen in the kidneys and ureters, although less frequent than in the bladder.
What cause bladder cancer?
Till date it is unclear what causes bladder cancer. A number of risk factors have been identified, but in many cases none of them may be present. (Risk factor is not a cause in itself but increases the risk that a cancer may occur). The risk factors are:
How is bladder cancer diagnosed?
Tests and procedures used to diagnose bladder cancer may include:
After confirming bladder cancer, additional tests may be recommended to determine whether the cancer has spread to your lymph nodes or to other areas of your body. These include:
What are the available treatment options?
Treatment options for bladder cancer depend on a number of factors, including the type of cancer, grade of the cancer and stage of the cancer, overall health of the affected individual and his treatment preferences
The options are:
• Surgery, to remove the cancer cells. Common types of surgery for bladder cancer are:
Surgery, to remove the cancer cells. Common types of surgery for bladder cancer are:
Transurethral resection of bladder tumor (TURBT). An endoscopic surgery to diagnose and remove cancers confined to the inner layers of the bladder, usually performed for cancers that aren't yet muscle-invasive cancers. This may be performed using laser technology.
Cystectomy. A surgery to remove all or part of the bladder that may be undertaken by open, laparoscopic or robotic technology. Partial cystectomy is a procedure where the surgeon removes only the portion of the bladder that contains a single cancerous tumor. Radical cystectomy is an operation to remove the entire bladder and the surrounding lymph nodes. After radical cystectomy a new way of urine storage and expulsion needs to be created using segments of intestine, called urinary diversion (different techniques are neobladder, ileal conduit, continent diversion).
A combination of treatment approaches may be recommended by your doctor and members of your care team.
What measures can be followed to reduce the risk of bladder cancer?
Although there's no guaranteed way to prevent bladder cancer, few steps can help to reduce bladder cancer risk.
Overview: Pediatric urology conditions include a wide range of conditions involving the genital and urinary tracts. Often these are congenital (present at birth) and diagnosed as early as prenatally or in infancy; in many cases, they are treated and resolved early in life, sometimes through surgical reconstruction. Other times, the conditions are acquired during childhood.
The most common condition seen by pediatric urologists is a urinary tract infection, which occurs more frequently in girls than in boys. An estimated 1-2 percent of children develop a UTI, characterized by blood in the urine, an unusual odor to the urine, or a change in urinary patterns. UTI in children can be associated with other congenital urological problems like vesicoureteral reflux, posterior urethral valve, megaureter and pelviureteric junction obstruction- so detailed evaluation is advised in all children.
A fluid-filled enlargement of the kidney prior to birth, typically diagnosed with prenatal ultrasound. It is seen in 1% of male pregnancies and 0.5% of female pregnancies. It may be due to blockage at the junction between the kidney and the tube that conveys urine from kidney to bladder (medically termed pelviureteric junction) or blockage at the junction between the tube and the bladder (medically termed the ureterovesical junction) or blockage at the level of urethra, the outlet from bladder to outside (a condition called posterior urethral valve). Depending upon the abnormality, ultrasound imaging may be needed throughout pregnancy and after a baby is born. In most cases, this diagnosis does not affect when, where or how a baby is delivered. Surgery is required in a small percentage of children during infancy and childhood.
A protrusion of all or part of an organ or tissue through a weakened area in the belly. The hernia creates a soft lump or bulge under the skin. When the hernia happens in the groin area, it is called an inguinal hernia. A hernia requires urgent surgical opinion and can be rectified using laparoscopic (keyhole) or open surgery. Laparoscopic surgery offers benefits like early recovery, less pain and cosmesis.
An accumulation of fluid that can occur in the scrotal sac. Up to 1 in 10 baby boys have a hydrocele at birth. In most cases, it goes away without treatment in the first year. A hydrocele that lasts longer than 12 to 18 months is often a communicating hydrocele. A hydrocele that lasts longer than 12 to 18 months is often a communicating hydrocele. This often needs surgery to prevent an inguinal hernia. Often surgery can be performed using laparoscopic (keyhole) technique with benefits like early recovery, less pain and cosmesis.
Swelling of the kidneys caused by obstruction in the urinary tract, detected after the child is born. The causes remain the same as Antenatal Hydronephrosis. Treatment depends on the disease condition and severity of the blockage.
A birth condition, usually diagnosed during infancy, in which the opening of the urethra (the tube that carries urine from the body) is on the underside of the penis rather than at the tip. Surgery usually restores the normal appearance of your child's penis. With successful treatment of hypospadias, most males can have normal urination and reproduction.
A disorder resulting from interference in the normal nerve pathways that send signals to the bladder regarding urination. It causes a child to have problems with holding or releasing urine. Many of these children also experience chronic constipation. The most common causes of this condition in a child are problems with the spinal cord. It can be diagnosed with urine tests, a urodynamic study, or an ultrasound. Common treatments for this condition include bladder training, bladder relaxing medications, surgery, intermittent catheterization (insertion of a tube to empty the bladder).
Bedwetting beyond the age at which a child would be expected to remain dry – believed to be caused by a developmental delay in the bladder and usually something the child outgrows. At five years of age, 15 to 25 percent of children wet the bed. With each year of maturity, the percentage of bed-wetters declines by 15 percent. 8 percent of 12-year-old boys and 4 percent of 12-year-old girls are enuretic; only 1 to 3 percent of adolescents are still wetting their bed. All children with bedwetting issues need detailed evaluation to rule out underlying disease conditions. Treatment options include Bladder Training, Medications, use of Bed-wetting Alarm.
Spina bifida – a neural tube defect in which the tissue surrounding the spinal cord fails to close properly during fetal development
A condition in which at least one testicle fails move into the scrotal sac as the male fetus develops. In about 10 percent cases, it may affect both sides. In some cases, the testis may descend by itself by 6 months after birth (especially in prematurely born babies). Surgery is usually recommended if it has not descended by 6 months and this is best adjudged by the pediatric urologist. The surgery may be performed by laparoscopy (keyhole) technique, with several advantages over open surgery. Early surgical treatment appears to lower the risk of later complications. In some cases, the testicle might be poorly developed, abnormal or dead tissue.
Blockage of the flow of urine in the area where the ureter meets the kidney. This usually leads to swelling of the affected kidney called hydronephrosis. All cases need consultation with pediatric urologist. Neglected obstruction or severe obstructions can lead to loss of the affected kidney function. The condition may require corrective surgery that may be performed through endoscopic, laparoscopic (keyhole) or open approach. The type of approach, depends on the disease severity and the surgeon’s expertise.
Vesicoureteral reflux is the abnormal flow of urine from the bladder back up the tubes (ureters) that connect the kidneys to the bladder. Normally, urine flows from your kidneys through the ureters down to your bladder in unidirectional manner.

It's not supposed to flow back up. The disorder increases the risk of urinary tract infections, which, if left untreated, can lead to kidney damage. Children with less severe vesicoureteral reflux are usually advised to take preventive antibiotics to avoid urine infection and consequent damage to kidneys. Children with severe reflux may require corrective surgery that may be performed through endoscopic, laparoscopic (keyhole) or open approach.
A condition where the foreskin is too tight to be pulled back over the head of the penis (glans). Phimosis is normal in babies and toddlers, but in older children it may be the result of a skin condition that has caused scarring. Phimosis is not usually a problem unless it causes symptoms such as redness, soreness or swelling. Surgery (circumcision) may be needed if the foreskin is painfully tight or the child experiences repeated episodes of local redness or scarring.
A condition where the urethral meatus (the opening of at the tip of the penis) becomes narrower. If the narrowing becomes significant, urine will trouble flowing from the bladder and may cause the bladder to not empty completely. If left untreated, this can lead to urinary tract infections and kidney problems. The corrective surgery is called Meatotomy and Meatoplasty.
Bladder procedures
Kidney procedures
Penis procedures
Testicle procedures
Ureter procedures
Urethra procedures
With Your Child in Mind
Our Center provides a comprehensive approach to pediatric urology care. Our goal is to minimize your child's discomfort and stress while streamlining the diagnostic and treatment process. In many cases, parents can obtain a treatment recommendation on their first visit. Our Center offers both diagnostic testing and open and minimally invasive treatment options
Minimally invasive treatment options in children
The two most commonly utilized minimally invasive treatment options are endoscopic (endourological) surgery and laparoscopic surgery.
Endoscopic (Endourological) Surgery
A surgical technique that involves specialized instruments that can enter the urinary tract via the urethra (the tube carrying urine from the bladder to outside the body), eliminating the need for incisions. The benefits are: No scars, Less Pain, Short Hospital Stay, Quicker return to activity. Disease conditions that can be approached through the urethra can be treated by this approach.
Laparoscopic Surgery
A surgical technique where the same surgery which was performed by open approach is performed through small openings in the child’s belly. Laparoscopy in children and adolescents bears marked similarities to adult procedures, but needs to be performed by pediatric urology expert trained in this technique. The benefits are: Less blood loss, Reduced risk of infection, Less pain, Smaller scars, Shorter hospital stay, Quicker return to activity.
What are common andrological conditions?
How does an Erection happen?
Erection is a psychological phenomenon in which the man’s penis raises from its natural level.
For a normal erection to happen,
The penis comprises two spongy tissue tubes, called “corpora cavernosa” surrounded by a tough fibrous-partially elastic outer casing, called “tunica albuginea”. When a man is aroused sexually, the blood vessels of the corpora cavernosa relax and open up and blood rushes in through the cavernosus arteries to fill the spongy tissues. The spongy tissues expand to accommodate the extra blood. The veins running over the outer case of the penis then compress obstructing the outflow of blood from the penis. As the blood is entrapped in the penis under high pressure, the penis swells within the outer casing, giving an erection. The pelvic muscles especially ischiocavernosus and bulbospongiosus also play a significant role in getting a good erection. Contractions of these muscles produce an increase in intracavernous (intrapenile) pressure and enhance penile rigidity (firmness). Erection is reversed when muscles in the penis contract, stopping the inflow of blood and opening outflow channels, and the penis becomes flaccid (soft).
How does Ejaculation occur?
Sexual stimulation and friction provide the impulses that are delivered to the spinal cord and into the brain. Ejaculation is a reflex action controlled by the central nervous system. It is triggered when the sexual act reaches a critical level of excitement. It has two phases.
There may come a time in any of our lives when our erections, which have often been frequent throughout our lives, begin to take a nosedive. Perhaps this has already begun to happen to you, in which case don’t worry: it genuinely is a fairly frequent problem.
What is erectile dysfunction (ED)?
“It is man’s inability to achieve or maintain an erection, suitable for satisfactory sexual intercourse.”
ED is also called impotence. It is the inability to engage in sexual intercourse. This condition can negatively impact any intimate relationship, not forgetting one’s psychological well-being too.
How Common is ED?
According to research, 150 million men suffer from erectile dysfunction and the number is doubling by 2025.
A survey showed that men over the age of 40 may experience at least one in five erectile problems and almost one in ten men is completely incapable of erections. With increasing age, each person is more likely to have erectile problems.
Causes of ED
ED can be caused by many physical or psychological factors. Some important causes are:
Nerve Damage
A proper nerve system is essential for normal erection. Men with neurological disorders may face ED. Common causes are:
Poor Blood Flow
Poor blood flow affects suitable erection. Common causes include:
Urological problems
Certain urological problems may lead to ED.
Interference by drugs, alcohol and medicines
Metabolic problems interfering with blood vessel function (endothelial dysfunction)
Psychosocial causes

ED- Common Questions:
Is ED a normal attribute of ageing?
No, erectile dysfunction has nothing to do with ageing.Is ED preventive?
By keeping healthy lifestyle and timely check on other health conditions you have, you can easily prevent erectile dysfunction.
Is ED hereditary?
No, erectile dysfunction is not hereditary.What is PELVIC FLOOR REHABILITATION (PFR)?
PFR is a therapy to reinforce your pelvic floor muscles which play a significant role in sustaining an erection. The experienced pelvic floor therapist, with the help of specialised equipment ensures stronger muscles especially ischiocavernosus and bulbospongiosus. These muscles lead to stronger erections and better ejaculations with the increase in Ejaculatory time.
What treatment options are available for ED?
The various treatment options are Oral Medications, Penile Injection Treatment, Low Intensity Shock Wave Lithotripsy, P-shot, External Devices, Penile Prsothesis
What is Low Intensity Shock Wave Lithotripsy (LI-ESWT)?
LI-ESWT is a novel modality that has recently been developed for treating ED. Li-ESWT induces tissue regeneration, neo-angiogenesis and improve endothelial function, thereby improving penile circulation. Apart from ED, it also benefits patients with Peyronie’s Disease and Chronic Prostatitis
what is PRP treatment
The PRP treatment or platelet rich plasma treatment as it is sometimes known, is a completely natural procedure that is non-surgical and painless. It involves the injection of platelet rich plasma into the shaft of the penis, once it has been sufficiently numbed. This attracts stem cells and growth factors that kick-start tissue growth in the nerves and blood vessels, that in turn improves the size and quality of your erections, thereby benefiting patients with ED as well as Peyronie’s Disease.
What external devices are available for erectile dysfunction?
Vaccum Erection Device is one such external device which is FDA approved and is easy and safe to use. In the process, tubular tubes or Vacuum devices are placed over the penis. As air is tapped out of the cylinder, and the pressure build-up helps to draw blood into the penis. This helps the penis to enlarge A rubber ring is then set around the bottom of the penis to maintain the erection.
What is a penile prosthesis?
A penile prosthesis is a pair of malleable (bendable) rods or inflatable rods (that may be inflated and deflated manually) that is surgically inserted into the penis. The Inflatable devices allow erections to happen by a mechanism of compressing on a special part by the device. Men disappointed with other treatments might opt for penile prosthesis implantation.

HOW TO IMPROVE ERECTIONS NATURALLY
According to The National Institute of Diabetes and Digestive and Kidney Diseases, certain foods should be avoided to achieve better erections:
Male infertility means not being able to father children. Infertility is the inability of a sexually active, non-contracepting couple to achieve spontaneous pregnancy in one year. If the cause of the fertility problem is found in the man, this is male infertility. In over a third of infertility cases, the problem is with the man. This is most often due to problems with his sperm production or with sperm delivery.
What Happens Under Normal Conditions?
The man's body makes tiny cells called sperm. During sex, ejaculation normally delivers the sperm into the woman's body.
The male reproductive system makes, stores, and transports sperm. Chemicals in man’s body called hormones control this. Sperm and male sex hormone (testosterone) are made in the 2 testicles, located in scrotum, the sac of skin below the penis. When the sperm leave the testicles, they go into a tube behind each testicle, called the epididymis.
Just before ejaculation, the sperm go from the epididymis into another set of tubes, called vas deferens. Each vas deferens traverses the scrotum, enters the abdomen and joins the ejaculatory duct and seminal vesicle behind the bladder in the pelvis. When ejaculation occur, the sperm mix with fluid from the prostate and seminal vesicles. This forms semen. Semen then travels through the urethra and out of the penis.
Male fertility depends on man’s body making normal sperm and delivering them. The sperm go into the female partner's vagina. The sperm travel through the woman’s cervix into her uterus to her fallopian tubes. There, if a sperm and egg meet, fertilization happens.
The system only works when genes, hormone levels and environmental conditions are right.
What are the common causes of male infertility?
Making mature, healthy sperm that can travel depends on many things. Problems can stop cells from growing into sperm. Problems can keep the sperm from reaching the egg. Even the temperature of the scrotum may affect fertility. The main causes of male infertility:
Sperm problems can be from traits a man is born with (genetic diseases). Lifestyle choices can lower sperm numbers. Smoking, drinking alcohol, and taking certain medications can lower sperm numbers. Other causes of low sperm numbers include long-term sickness (such as kidney failure), childhood infections (such as mumps), and chromosome or hormone problems (such as low testosterone).
Damage to the reproductive system can cause low or no sperm. About 4 out of every 10 men with total lack of sperm (azoospermia) have an obstruction (blockage) within the tubes the sperm travel through. A birth defect or a problem such as an infection can cause a blockage.
Other causes of Male Infertility are:
What are the common diagnostic tests?
Causes of male fertility can be hard to diagnose. The problems are most often with sperm production or delivery. Diagnosis starts with a full history and physical exam. Other commonly utilized diagnostic tests are:
What treatment options are available?
Treatment depends on what's causing infertility. Many problems can be fixed with drugs or surgery. This would allow conception through normal sex. In certain cases with no response to medical treatment or when surgery is not feasible (unknown causes of male infertility), sperm harvest from the testis and assisted reproduction techniques (IVF) may be required.
Frequently Asked Questions on Male Infertility
What health problems can cause male infertility?
Many health problems--from kidney disease to testicular cancer--can result in male infertility. "Whole-body" health problems and metabolic disorders, and ordinary fevers and infections can harm sperm growth. Diseases passed through sex can lead to blocks and scars in the reproductive tract.
Genetic health problems, such as cystic fibrosis can cause the vas deferens or seminal vesicles to be absent leading to no sperm in the semen. Many illnesses can cause infertility. It's important that you and your partner tell your family and personal health histories to your health care provider.
Can cigarette smoke affect sperm?
Yes. Research shows that routine smoking affects sperm in many ways. It causes sperm cells to be smaller and slower. It harms their DNA. Smoking can also affect the seminal fluid ejaculated with sperm.
Can using steroids for body building cause infertility?
Yes. Steroids taken by mouth or shot can cause your body to stop making the hormones needed to make sperm.
Do abnormal semen analyses or sperm lead to children with birth defects?
Not necessarily. For most couples seeking fertility treatment, the risk of conceiving a child with a birth defect is the same as for the general population. Some problems (chiefly genetic problems) that cause infertility may also cause a greater risk of conceiving a child with birth defects. So couples need thorough exams and advice before beginning some forms of ARTs.
What's the main thing I should know about male infertility?
Infertility is not your or your partner's fault. The American Society of Reproductive Medicine (ASRM) estimates that in about a third of infertility cases it is due to the male. Another third is the female.
In the last third of infertile couples, the problem is caused by either a combination of reasons, or, in 20 out of 100 cases, it can't be explained. In men, few or no sperm is the biggest problem. In women, the common problems are ovulation problems and blocked tubes. But today, technology and surgical tools exist to address many of these problems.
Vasectomy is a safe, effective, and permanent method of contraception. It should be considered in men who wish for:

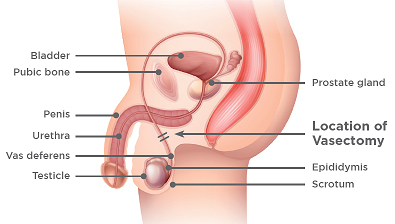
What is a Vasectomy?
Sperm are produced in the testicles before moving into the epididymis, which sits on the back surface of each testicle. These sperm remain in the epididymis where they mature. The sperm then travels up each vas and are expelled at the time of ejaculation in the semen.
When a vasectomy is performed, the vas deferens are cut and sealed, preventing sperm from leaving the epididymis. This way, no sperm are expelled from the penis at the time of ejaculation.
If you would like more specific information on Vasectomy please view one of the following pages. If what you are looking for is not there, please don’t hesitate to give us a call today. We are more than happy to help you & educate you.
Vasectomy success rates
Vasectomy is successful in more than 99 percent of men. Other methods of contraception are required until a semen analysis confirms there are no sperm in the semen.
The sperm count is checked approximately three months after the procedure. A man needs to have had at least 20 ejaculations after vasectomy to clear the ducts of sperm.
If the semen analysis shows sperm that do not move there is a small chance that a pregnancy may occur. Other methods of contraception should be continued until a clear test result is completed
Vasectomy Procedure
Men who are considering a vasectomy have a consultation before the procedure. At this appointment, the doctor will explain the procedure and answer any questions.
Vasectomies can be performed under a local or general anaesthetic. There will be a small scar from the incision but this will not be very noticeable once it has healed.
After the Procedure
You may go home shortly after your procedure. Preferably someone else should drive you home.
Pain control following Vasectomy
After the vasectomy, there may be some discomfort at the incision site. This can be relieved with a pain medication such as paracetamol. Ibuprofen and aspirin should be avoided for at least one week to minimise the risk of bruising and bleeding around the incision.
Semen tests
You are not clear to discontinue the use of other forms of contraception until you have been formally advised that you have achieved a zero sperm count at least three months and a minimum of 20 ejaculations following surgery.
Health effects of Vasectomy
Sex drive
Having a vasectomy will not affect testosterone levels, sex drive, or the ability to have an erection.
Risk of cancer
Although there have been some concerns regarding a link between vasectomy and prostate and testicular cancer, several large studies suggest that there is no increased risk of any cancer. Heart disease – similar to the situation with cancer, despite some concerns, studies have not found any link between vasectomy and heart disease.
Contraception after a vasectomy
If the semen analysis shows no evidence of sperm you may discontinue the use of other forms of contraception. Vasectomy does not protect against sexually transmitted diseases such as HIV.
Urodynamic testing is often used to try and find out what is causing bladder problems. It is the study of the bladder’s ability to hold and empty urine. It measures the way the bladder relaxes to fill and then contracts to empty. The evaluation is assisted with a computerised study.
Allow a total appointment time of one and a half hours for test and review by the doctor.
Before the Procedure
During the Procedure
After The Procedure
A prostate biopsy is a safe and effective sampling technique during which tissue is obtained from the prostate gland for the purpose of detecting cancer.
Trans rectal ultrasound guided biopsy is the preferred approach in most cases. It involves the examination of the prostate by an ultrasound probe inserted into the rectum. After local anaesthetic has been injected, a fine needle is inserted into the prostate and a number of small samples (biopsies) are taken.
Allow a total appointment time of 30 minutes, although the procedure itself normally takes 5-10 minutes.
Before the procedure
During the procedure
After the procedure
Risks and complications
Infection
If you feel unwell with a headache, sweating, fevers, chills, painful testicles or problems passing urine, you need to contact your Urologist immediately as you may require admission to hospital for further treatment.
Bleeding
You may experience blood in your urine, bowel motion and semen and this will gradually subside over the next 2 weeks and rarely causes a problem. If bleeding persists or is very heavy, contact your doctor.
Inability to urinate
This can occur due to swelling around the prostate and may rarely lead to a complete blockage of urine flow. If this occurs, contact your doctor.
Pain and discomfort
You may experience discomfort in the rectum or base of the penis. This is very common and should settle within 24-48 hours.
What is Laparoscopic surgery?
Laparoscopic surgery (‘keyhole’ or ‘minimally invasive’ surgery) is the technique of performing surgery through multiple small incisions, rather than one large incision Through these small incisions, ‘ports’ are placed to pass a telescope, light source, and instruments, and carbon dioxide is used to inflate an operating ‘workspace’.
Advantages
Disadvantages
What is a laparoscopic nephrectomy?
This procedure involves removing the kidney through ‘key hole’ surgery. The procedure is most commonly performed to remove cancer but may be indicated to remove a kidney severely damaged by obstruction, stones, or infection. The procedure is performed through 3 or 4 incisions in the front of the abdomen, or the back, depending on specific technique used. If the kidney is removed for cancer, one incision is enlarged to 6 – 8 cm to allow removal of the kidney intact for further analysis. If it is too difficult to complete the surgery laparoscopically, a larger cut is made to remove the kidney through more traditional open surgery. This is necessary in around 5% of cases.How long does it take?
3-4 hours under a general anaestheticWhat are the risks?
What can I expect after surgery?
Living with one kidney
One kidney can easily support a normal and active life. There is no need to limit activities or lifestyle.
What is a laparoscopic pyeloplasty?
This is an operation to remove the blockage between the outlet of the kidney (renal pelvis) and the kidney tube (ureter). This condition is called pelvi-ureteric junction (PUJ) obstruction. This blockage is mostly due to a blockage that occurs from birth, due to abnormal development of the kidney. Rarely it can be due to the previous scarring that narrows the tube, caused by stones, trauma or previous surgery.
Key-hole surgery is performed through 3 – 4 incisions through the side of the abdomen to remove the blockage. A small tube (stent) is left in the ureter for 4-6 weeks to allow the tube to heal. This is then removed under local anaesthetic by passing a small telescope (cystoscope) into the bladder.
Conversion to a conventional open operation can occur if the procedure can not be performed through key-hole surgery. This occurs in approximately 5% of cases.
Why do I need this?
The operation is needed if the blockage causes kidney pain, kidney infections or the kidney function becomes damaged. It can also be associated with kidney stones and high blood pressure.
How long does it take?
4-5 hours under a general anaesthetic
What are the risks?
What can I expect after surgery?
What is Ureteroscopy?
Why do I need this?
You have a stone in your ureter, less than 2 cm in size, which may be causing pain, obstruction, bleeding or infection
How long does it take?
30 – 60 minutes under a general anesthetic, depending on the stone size, location, and hardness
What are the risks?
What can I expect after surgery?
The following day, any catheter if placed, is removed and you can go home once you have passed urine
What is TURBT?
Why do I need this?
To remove a bladder tumor and determine if it is a cancer and its extent
How long does it take?
20 – 40 minutes under a general anaesthetic
What are the risks?
What can I expect after surgery?
Bladder Cancer Patient Guidebook
Canadian Patient Guidebooks - Downloads - Bladder Cancerhttps://bladdercancercanada.org › canadian-patient-guide
What is a ‘TURP’?
How long does it take?
What do I need to do before surgery?
What are the risks?
What can I expect after surgery?
Holmium Laser Enucleation of the prostate (HoLEP) is a modern alternative to the standard Transurethral Resection of the Prostate (TURP) procedure for bladder outflow obstruction due to BPH. It requires a short period of hospitalisation and a general anaesthetic. A catheter (a tube which drains the bladder) is required for 1-2 days until the urine is clear. Patients are advised to take life quietly and to avoid straining or heavy lifting for four weeks after the surgery.
Who is it suitable for?
What does the procedure involve?
A laser is used to help remove tissue from the prostate gland which is causing a restriction to the flow of urine out of the bladder.
What are the advantages of HoLEP?
What problems can occur after surgery?
Common (greater than 1 in 10)
• Temporary burning, bleeding and frequency of urination
• No semen produced with orgasm (75 out of 100 men) - permanent
• Not all urinary symptoms may resolve
• Infection of bladder, testes or kidneys
• Failure to pass urine requiring temporary catheter placement
Occasional side-effects (1 in 10 to 1 in 50)
• Loss of urinary control
• Damage to erections
• Injury to urethra (water-pipe) causing scarring, further operation may be required
• Finding of unsuspected cancer in the tissue removed from the prostate
Rare side-effects (less than 1 in 50)
• Repeated treatment for re-growth of prostate gland (1% at seven years)
• Self-catheterisation or indwelling catheter if bladder is weak
• Ongoing loss of urinary control (incontinence), further operation may be required (less than 1%)
• Retained tissue fragments in bladder, may require telescopic procedure
• Injury to ureter (drainage tube from kidney)
• Perforation of bladder needing further surgery
• Bleeding requiring return to operating theatre
Your Urologist will be happy to discuss HoLEP with you.
What is an insertion of penile implant?
Why do I need this?
This procedure is reserved for severe erectile dysfunction where sexual intercourse is not possible and other treatments have failed or are unsuitable
How long does it take?
90 – 120 minutes under a general anaestheticWhat are the risks?
What can I expect after surgery?
